
Livonia, MI – When a document prepares arranges documentation for a rehabilitation provider, this must be based upon what the treating therapist communicates. This includes goal setting. This item provides a basis for determining what the therapist should communicate.
Then the document prepares takes those s notes and prepares service documentation. At the end of this article is a form that could be used for a therapist to quickly provide information each time a session is conducted or a provider may have a digital system to use for this purpose.
An accurate flow of information creates integrity and makes you audit proof. That matters!
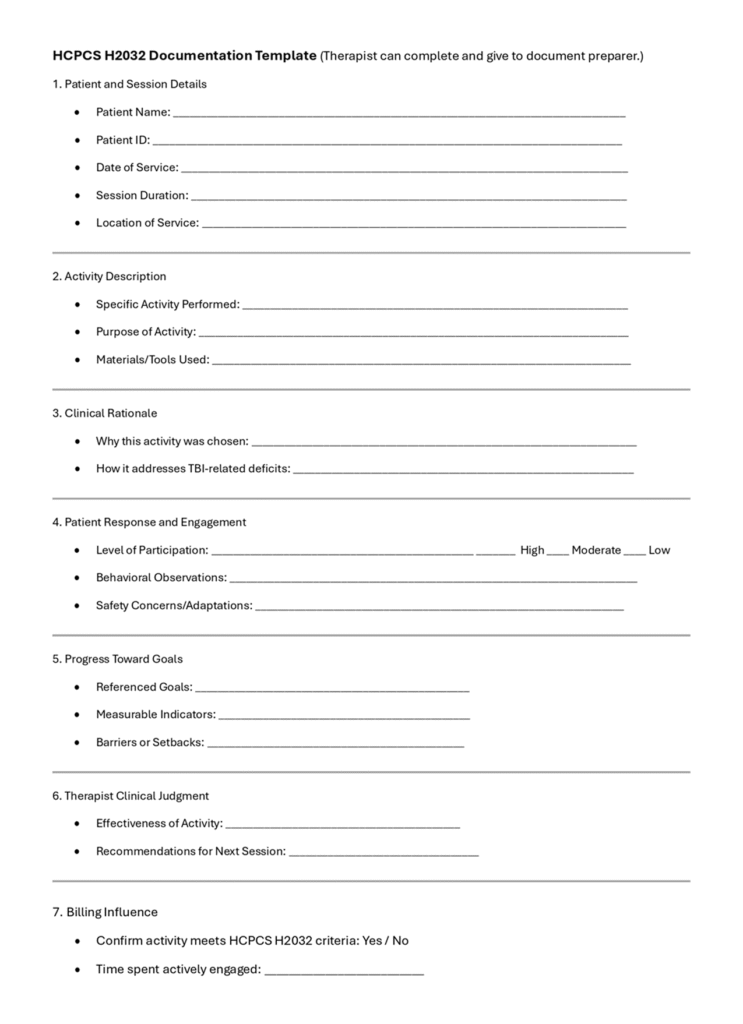
1. Patient Identification and Session Details
- Date, time, and duration of the session.
- Patient name and unique identifier.
- Location of service (inpatient, outpatient, community setting).
2. Therapeutic Activity Description
- Specific activity performed (e.g., cognitive sequencing task, fine motor coordination exercise).
- Purpose of the activity in relation to rehabilitation goals.
- Materials or tools used during the activity.

3. Clinical Rationale
- Why this activity was chosen for this patient.
- How it addresses functional deficits related to TBI (e.g., attention, memory, executive functioning).
4. Patient Response and Engagement
- Level of participation (active, minimal, required cues).
- Behavioral observations (e.g., frustration tolerance, problem-solving ability).
- Safety concerns or adaptations made during the session.
5. Progress Toward Goals
- Specific goals referenced (e.g., “Improve ability to follow 3-step commands”).
- Measurable indicators of progress (e.g., “Completed 4 out of 5 steps independently”).
- Any barriers or setbacks noted.
6. Therapist’s Clinical Judgment
- Assessment of effectiveness of the activity.
- Recommendations for next session or modifications needed.
7. Billing Influence
- Confirmation that the activity meets criteria for H2032 (structured, therapeutic, goal-directed).
- Time spent actively engaged in therapy (not prep or idle time).

Why the Therapist Must Influence the Summary
- Compliance: Only the therapist can ensure the documentation reflects skilled intervention rather than recreational activity.
- Medical Necessity: Payers require evidence that the service was clinically justified and goal-oriented.
- Accuracy: Misrepresentation or vague summaries can lead to claim denials or audits.
- Ethical Standards: Therapist input prevents fraudulent or misleading documentation.
Warnings for Document Preparers:
1. Avoid a Cut-and-Paste Approach
- Repetitive or boilerplate notes raise red flags with reimbursement sources and auditors.
2. Tell a Story
- Documentation should narrate the therapeutic process, not just list tasks.
3. Never State “Patient is Moving Toward Goals” Without Details
- Always specify what the goals are and how progress was demonstrated.
4. Do Not Omit Clinical Rationale
- Activities must be linked to functional improvement, not just described as “fun” or “engaging.”
Important Warnings for Document Preparers:
- Avoid a cut-and-paste approach; repetitive notes raise red flags.
- Tell a story; narrate the therapeutic process, not just list tasks.
- Never state “Patient is moving toward goals” without specifying goals.
- Do not omit clinical rationale; link activities to functional improvement.

Another Blog Post by Direct Care Training & Resource Center, Inc. Photos used are designed to complement the written content. They do not imply a relationship with or endorsement by any individual nor entity and may belong to their respective copyright holders.
| Follow us in the Social Stratosphere… | ||||
|
|





